
15 Jan Why Myofascial Release Doesn’t Work for Chronic Pain
Myofascial release is well-intentioned.
“Let’s get rid of the pain.”
But good intentions don’t mean good results.

After all, it was Adam Grant in Jurassic Park 3 who said:
Some of the worst things imaginable have been done with the best intentions.
Now, you might be thinking:
“That’s a bit of a stretch. Worst things imaginable? Just by getting some myofascial release therapy done?
Yeah, it’s not OK that people in chronic pain don’t get the care they deserve.
Here’s a list of things that can go wrong with myofascial release when it’s not addressing the CAUSE of your chronic pain:
- You DO NOT get diagnosed correctly and DO NOT get treatment that you need … making your chronic pain worse.
- You waste time, money, and energy that lets your joints degenerate further.
- Your joint degeneration gets worse, which means a lesser percentage of permanent pain relief is possible.
- Once your joint degeneration is worse, the pain can only be managed in a 24-48 hour window with things like CBD, massage, myofascial release, acupuncture, physical therapy, or chiropractic adjustments.
What’s the Goal of Myofascial Release?
Google “myofascial release.”
10,000 to 100,000 people google it each month.

At the time of the writing of this post, the 2nd post down will bring you to Healthline.
I’m sorry, but no, Healthline.
Pushing on trigger points may work for acute pain that lasted a day or two, but it will not work for people with chronic pain that has lasted more than 6 months.
We already wrote about trigger points, or muscle knots and the Great Spaghetti Phenomenon of the 21st century.
Trigger points and muscle knots are secondary problems.
They are the effect.
Not the cause.
The only way to get permanent relief from chronic pain is to treat the primary problem.
The cause.
That means treating fibrous adhesion, which is kinda like glue in around your muscles, ligaments, tendons, and nerves.
Adhesion is a VERY different problem and feels very different than trigger points.
Adhesion is Kinda Like Glue In Your Muscles
Even surgeons are starting to recognize adhesion or “no name bands” as a culprit of chronic pain and nerve entrapments like carpal tunnel syndrome or pronator teres syndrome.
Check out this surgery releasing adhesion from the median nerve in the forearm.
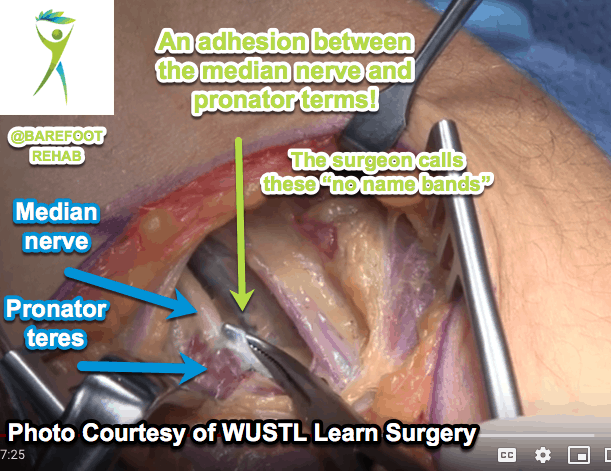
Adhesion is that spider-webby, gluey, white stuff in the surgeon’s instrument.
A scalpel is one way to remove adhesion.
Another way to remove adhesion is with a tension force, non-surgically.
The white stuff in the below image is fascia.
Healthy fascia is less dense.
When adhesion thickens and snowballs (getting bigger), it becomes fibrous adhesion.
In the below diagram, fascia is stacked vertically and attached to two force plates.
See the 1st image all the way on the left. It looks like a WHITE letter “I”.
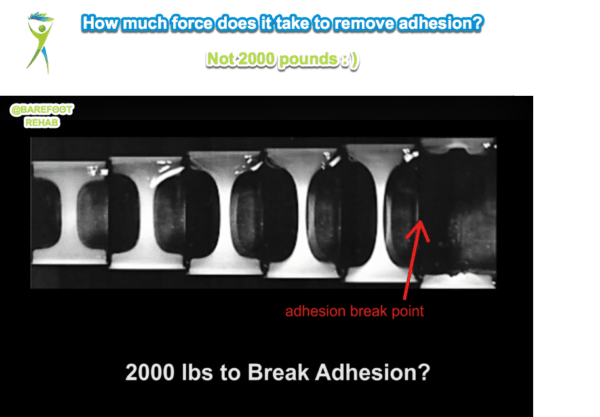
Each successive image to the right is pulling the fascia apart further, thinning out the fascia …
… til it breaks in the image all the way to the right.
Adhesion ONLY breaks when you put a tension force, pulling the adhesion apart.
Not even an elephant can break adhesion by standing on it!
Why Myofascial Release Doesn’t Work for Chronic Pain
Imagine a rubber band on the floor.
Have an elephant stand on it.
See the elephant standing on just one foot on that dainty little rubber band.
This is a compression, or downward, force.
When the elephant gets off the rubber band, is it intact?
Most people can perceive that the rubber band will still be able to bundle a newspaper.
Compression doesn’t break adhesion.
Now, have a 5 year old child pick up the rubber band and pull it apart.
Did it snap?
You bet it did!
This is a tension, “pulling apart”, force.
Tension is what breaks adhesion.
Sure, you can use a scalpel.
But do you really want to get cut open when you don’t need to?
What Non-Surgical Technique DOES Work to Break Adhesion?
Manual Adhesion Release (MAR) is the chosen technique for breaking fibrous adhesion.
It is taught by Dr. William Brady of Integrative Diagnosis.
You can find a provider who practices this technique through Integrative Diagnosis’s Find a Provider page.
Here’s what how an MAR provider sets up to remove fibrous adhesion from a patient’s low back.
This is what it looks like from the side.
Then, even if your joints are severely damaged, you can potentially avoid surgery on your low back like Natalie did.
Or like Anthony avoided shoulder surgery for his torn labrum by getting adhesion removed from his rotator cuff:
Or like Jasmine avoided a neck fusion by getting the adhesion removed from her neck:
Where’s the Best Place to Get Your Chronic Pain Treated?
The best place to get your adhesion removed when your pain has:
- lasted more than 6 months
- you’ve seen at least 3 doctors or myofascial release therapists
… is Barefoot Rehab in Denville, NJ.
We’re currently the ONLY practice in the United States with non-surgical pain specialists who treat by BODY REGION.
Why would you want to see a chronic pain chiropractor, physical therapist, or myofascial release therapist who treats pain in the whole body when you can get treated by someone who treats:
- necks
- arms
- legs
- low backs
… all day, every day?
You’d never see a surgeon who operates on the whole body.
At Barefoot Rehab, we believe the standard for non-surgical care should be the same as surgeons.
If you think you might be a candidate for the PERMANENT pain relief we offer at Barefoot Rehab, give us a call at 862-205-4847 to speak with one of our patient advocates and take the next steps and see if you qualify!
 What has your experience been with myofascial release? Have you gotten any permanent pain relief from your chronic pain?
What has your experience been with myofascial release? Have you gotten any permanent pain relief from your chronic pain?

Jason
Posted at 15:02h, 05 AprilThat’s good stuff but with all due respect to MAR as a distinct modality, it’s been around in many different pin and stretch style techniques including Rossiter, Rolfing, Structural Integration, Active/Passive deep myofascial techniques, etc. A suggestion: I would seriously reconsider using the thumb )as used in the first video of this post) generally for even mild compression work but if you need to, support it with the index finger pressing at the distal interphalangeal joint to minimize hyperextension and overuse syndromes. A soft fist, palm or proximal ulna can perform that function with minimal impact on the body.
Dr. Chris
Posted at 15:24h, 05 AprilHi Jason! TY so much for your comment.
Unfortunately, many of our patients have tried all of the techniques you described with no or minimal relief. And they get much greater jumps of relief with us. Because we don’t take patients who have seen less than 3 doctors, we see a lot of what doesn’t work for patients.
I’ve been wanting to film FB and IG lives with another doctor who claims that their techniques, like you describe, is as effective as MAR. If you know anyone willing to film this with me because they belief they’re delivering the same value we are, please tell them. I’d even be willing to throw $10k in a pool to see who gets faster (AND PERMANENT) range and symptom improvements! The reason I’m willing to do this is to put skin in the game so I can show how strongly I believe that MAR is the most effective adhesion release.
I know this sounds elitist, but I can’t think of any other way to show practitioners so patients get the care they deserve. If someone made this offer to me, I would jump at it!
Again, forgive me, I’m not trying to point the finger. Only trying to raise the game in myofascial work. : ) Humbly, Chris.