
19 Jan The Truth About Plantar Fasciitis (and Arch Pain)
Does the bottom of your foot hurt or even burn?
Then you may have plantar fasciosis. (Notice I didn’t say plantar fasciitis.)
Like Janice did.
Why It’s Not “Plantar Fasciitis“
The “-itis” ending for tendonitis or fasciitis implies “inflammation.”
Plantar fasciitis is usually diagnosed under two conditions:
- Location – plantar foot (usually at the calcaneus attachment point).
- Symptom – pain that is worse with activity.
Inflammation is the natural bodily process of attempting to heal. It is normal and healthy in musculoskeletal conditions such as a bruise on the arm or a torn hamstring. When the immune system is busy trying to clean up your mess and you try to use the damaged tissue, your nervous system will let you know it’s angry at you with your subjective experience of “pain”.
Inflammation isn’t normal when the body is in a hyper-inflammatory (“hyper”= too much), usually through a diet consisting of grains, processed or low-fat dairy, and sugar, but that’s for another time.
The hallmark signs of inflammation are:
- rubor – redness
- tumor – swelling
- calor – heat
- dolor – pain
In most diagnoses of “plantar fasciitis”, the only hallmark sign of inflammation that is present is pain. There is no redness, swelling, or heat present. With one out of four signs of inflammation present, it makes one wonder “If it’s not fasciitis, what is going on?”
Plantar fasciosis, different from plantar fasciitis, is diagnosed under two conditions:
- Location – plantar foot (usually at the calcaneus attachment point), in the same location that plantar fasciitis would occur.
- Symptom – pain that in the early phases of degeneration, would get better with activity.
Notice the very clear difference concerning when the pathology is provoked. In fasciitis, activity makes the symptoms worse. In fasciosis, activity makes the symptoms better (as long as the degeneration is in the early stages). In the later stages of fasciosis, symptoms will be provoked with activity and will resemble fasciitis.
The difference between diagnoses cannot be overstated for symptom resolution.
What is fasciosis?
Fasciitis is an acute overload of the fascia.
Fasciosis (or degeneration) is the chronic overload of the fascia.
Chronic overload is due to:
- overload of healthy tissue (too much work) in the short-term … or …
- overload of underloaded tissue (not enough work in long-term that causes tissue to weaken then degenerate with too much work) over time.
When researchers open up the fascia in anatomical studies, they don’t find inflammatory cells in the face of this chronic overload.
What do they find?
Observe the window of a box of spaghetti. Notice all of the spaghetti are lined parallel to eachother, straight up and down.
{kind=link}
This is how the fibers are oriented in a normal, healthy tendon. One that can handle the load you put on it.
Now take the box of spaghetti and cook it or worse, throw it on the ground (and waste it). After either event, the spaghetti will no longer be parallel, but going in every direction.
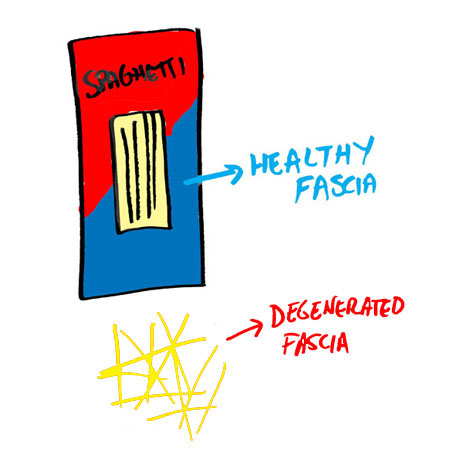
This is how the fibers are oriented in a degenerated tendon. One that can’t handle the load you put on it (and lets you know that the fire alarm is going off with “pain”).
Conventional Management of Plantar Fasciitis (and Arch Pain)
As mentioned above, degeneration in the plantar fascia occurs by doing too much or too little work.
It can develop in a runner who does fifty miles a day or in a tv-watcher who watches fifty tv shows a day.
With a diagnosis, Wikipedia’s list of treatments for plantar fasciitis (and arch pain) includes:
- rest
- massage therapy
- stretching
- weight loss
- night splints
- motion control running shoes
- physical therapy
- Cold therapy
- orthotics
- anti-inflammatory medications
- injection of corticosteroids
- surgery
Two data points(location and symptom provocation) are often correct to diagnose plantar fasciosis. The issue with this list of treatments is that it does not address the cause of the problem, only a plethora of random solutions that have potentially worked with the whole spectrum of plantar diagnoses, not your individual body.
Let’s look at the list again and discuss the dysfunction blocks that the solution points to.
- rest – implies “acute inflammation” of plantar fascia, and is only helpful when the tissue was healthy before the incident.
- massage therapy – implies a “soft tissue problem”, but is largely ineffective at removing scar tissue.
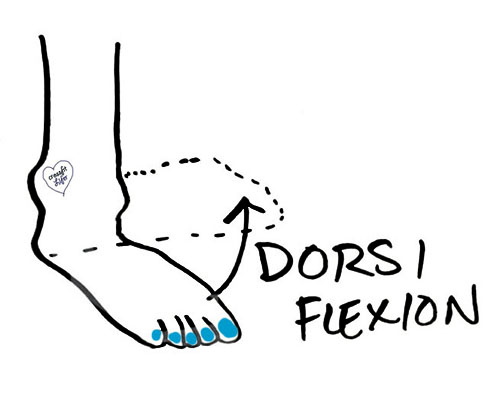
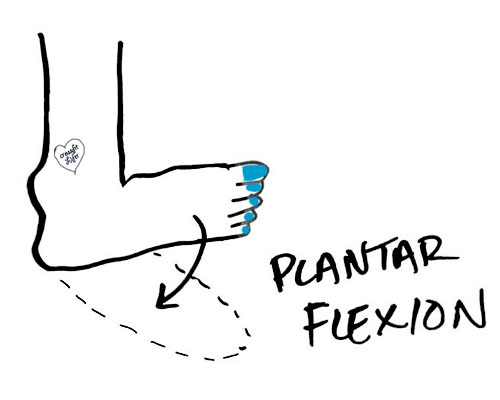
- stretching – implies “tightness”, which is often very true with restricted ankle dorsiflexion and plantar flexion (see below – Measure your ankle dorsiflexion through the directions here). Tissues can be tight for various reasons that warrant further detail to resolve (ie. muscle tightness from disuse, “protective tightness” from the nervous system due to local pathology, “increased tone” from the nervous system due to systemic pathology, etc.). The gross ineffectiveness of this solution is observed with the duration, in months to years, that individuals try stretching without actual feeling more flexible.
- weight loss – implies “increased load from standing or walking” is a problem. It can be, but it isn’t first priority.
- night splints – see the rationale for “stretching” from above.
- motion control running shoes – this intervention assumes pronation or supination need to be controlled. This is a valid point and a priority, just not priority one.
- physical therapy – implies that “weakness” is a problem. Weakness is often involved, especially when symptoms are bilateral. If this were priority one, physical therapists would be hitting home runs every time with this problem. They aren’t.
- Cold therapy – implies “inflammation” is a problem. But we’ve already clarified how plantar fasciitis is not caused by inflammation, it is plantar fasciosis caused by degeneration.
- orthotics – implies “faulty bone structure and alignment”. Definitely a priority that needs to be addressed. Unfortunately, most orthotics are garbage. We use Sole Supports (as does my mentor and the community of chiropractors he continues to teach) and get great results with them.
- anti-inflammatory medications – implies “inflammation” is a problem. See intervention cold therapy from above.
- injection of corticosteroids – implies “acute inflammation.” See rest from above.
- surgery – implies “something needs to be cut out or removed.” Whoa, what are you cutting Mr. Ortho?!
The Successful, Unconventional Treatment of Plantar Fasciosis
If the interventions above worked, patients wouldn’t go from podiatrist to podiatrist, year after year, looking for answers as many of our patients do.
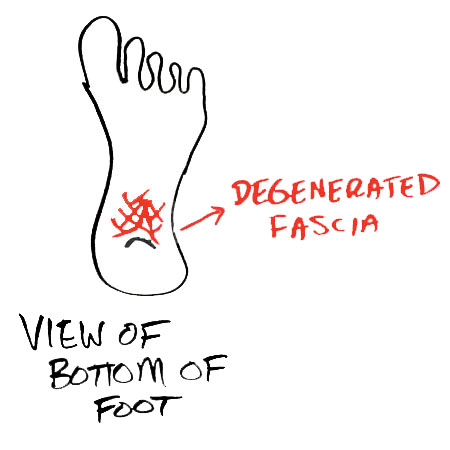
The NUMBER 1 problem in plantar fasciosis is the adhesion that develops in the calf (tibialis posterior, flexor hallucis longus, flexor digitorum longus) and foot (more than 30 tissues exist in the bottom of the foot) and the degeneration that occurs in the plantar fascia as the fibers are oriented in a haphazard fashion. You can learn if you have scar tissue in these structures by self-assessing your ankle dorsiflexion range of motion.
Legitimate secondary problems are non-optimal bone alignment, high-load activities of daily living, excessive mental and emotional stress, and systemic inflammation through diet or environmental toxins.
Knowing what all of these problems are, a sweet spot solution needs to be delivered for each individual problem.
- The NUMBER 1 solution for plantar fasciosis: a myofascial treatment that reduces the amount of adhesion in 1-5 visits, as observed in a Test-Treat-Retest Metholodgy of Treatment. My personal opinion is that an Integrative Diagnosis provider offering Manual Adhesion Release is the best choice for quick and permanent results. The plantar foot is also one place where instruments such as Graston work very well, but it can only be used on superficial tissue. Graston would not work well on the deep calf structures.
- Orthotics – to correct bone aligment between the second metatarsal and the tibia. As much as I used to believe that everyone should be walking around barefoot, faulty bone structure proves this belief wrong. I learned this the hard way through destroying my own ankle with barefoot running.
- Modification of Activities of Daily Living –the body needs to be loaded just the right amount to be healthy. Overload (running too much without sufficient time for recovery) or underload (sitting for eight hours a day) won’t keep the spaghetti lined up nicely in the box. Only in introducing movements such as squats and lunges into an exercise program, taking breaks from sitting, managing the amount of running one days we can prevent this problem from developing in the future.
Here’s the big picture: if you have plantar fasciosis and you’re not getting the scar tissue addressed through manual therapy, you’re not addressing the main problem. Your symptoms may go away with Wikipedia’s interventions, but I’m confident in saying they will return.
You can find providers near you by clicking on the appropriate link: Integrative Diagnosis, Active Release Technique, Graston Technique, and Sole Supports.
 Comment below: How long have your chronic plantar foot symptoms lasted? And how many different providers have you tried to get the right diagnosis?
Comment below: How long have your chronic plantar foot symptoms lasted? And how many different providers have you tried to get the right diagnosis?

Case Study: Frozen Shoulder Success
Posted at 15:47h, 28 January[…] I’ve already written how I don’t care about your herniated disc and the truth about plantar fasciitis. […]
The Truth About Achilles Tendinitis
Posted at 14:42h, 01 February[…] I already wrote about the difference between fasciitis and fasciosis in the plantar fasciitis post. […]
The Truth About Achilles Tendinitis (And Achilles Pain)
Posted at 14:44h, 01 February[…] I already wrote about the difference between fasciitis and fasciosis in the plantar fasciitis post. […]
Avoid the Most Common Running Injuries
Posted at 14:56h, 10 July[…] plantar fasciitis […]
Dareau Debrecen
Posted at 14:09h, 10 JanuaryI had been wearing shoes with a small heel for about 6 months. I then bought some ‘nice’ walking shoes with comfy insoles (no heel). After a week, I had what felt like a cramp in the arch of my right foot. It went away with rest. It happened four or five more times to the arch of my right foot over the course of a month. It felt tight. Then the pain in the arch of my right foot became acute. Then a few days later it developed in my left foot even though I hadn’t left the house at all in two days. Things took a turn for the worse very quickly. I can’t walk at a normal speed. I have to walk slowly or else I get tears in the fascia. I know, because I feel a sharp, cutting like feeling when it happens. When the tears occur, my foot will swell. The arch of both feet is so incredibly sensitive that I can’t even step on the edge of a carpet (an uneven surface) without it hurting me. I can’t massage or press the arch of my foot against anything, even a blanket without experiencing pain and subsequent swelling that could last hours or a whole day. I recognised what may have happened, my heeled shoes left the muscles and fascia of my arch very weak as the arch of my foot never touched anything while wearing the heels. I got another pair of heeled shoes though, as I thought this would relieve the pressure on my arch. It did. It’s the only way I can walk at all since every other shoe or being bare foot cause surfaces I step on to press against my arch causing tears in the fascia. It’s been about a month already. There’s no sign whatsoever that it’s ever going to get better. I used to walk for hours everyday, and dance, and now I can’t walk for more than 25 minutes at a time (slowly with a walking stick) without risking tearing the fascia further. I felt scar tissue forming in my right foot as I could feel it stretch especially in the morning when I flexed my foot both ways. But I did this gently and the stretching feeling of the scar tissue in the arch of my right foot is minimal now compared to what it was. I am afraid it may denigrate to the point of my no longer being able to walk at all. Oh and I should mention, it’s only pain in the arch of my foot, not in the heel at all. And nearly every article I find talks about heel pain. They also talk about “getting back to running” which is laughable since I gave up running 4 years ago. I don’t give a shit if I can never run, I want to fucking walk like a normal person again.
I see recovery times of 6 months to 1 and half years, but there’s no indication as to how bad the symptoms were for people at the start, or how they diminish in that period of time. Considering most people talk about, running through the pain or some such nonsense I am forced to believe my condition is very different or very very serious.
Can someone let me know if they’ve heard of a case as bad as mine before?
Dr. Chris
Posted at 15:42h, 10 JanuaryHi Dareau, yes, I’ve seen bad cases like yours. A few, I was able to get better and get back to walking. Other, after about 5-10 treatments and an MRI that confirmed significant tearing or tendon degeneration, I referred surgery.
But you’re correct, you don’t have plantar fasciitis. You likely have adhesion in the bottom of your foot and/or tendon degeneration that is responsible for your pain.
Honestly, it depends on all of the variables that are contributing to your foot pain.
ADHESION – most commonly, do you have adhesion in the back of your calf, front of your shin, and bottom of your foot? (You can test yourself here: https://www.barefootrehab.com/know-your-numbers-ankle-pain-foot-pain-and-ankle-dorsiflexion/)
WEAKNESS – are your muscles weak?
PATHOLOGIES – what does an MRI say as far as pain-producing tissues
OTHER METABOLIC CONDITIONS – do you have diabetes, a thyroid condition, or some other immune system compromising problem?
Some things I’m curious about:
AGE – how old are you?
LX – where do you live?
OTHER HX – have you had other pain issues from the low back on down?
Let me know and I’ll do the best I can to support you.
Dareau Debrecen
Posted at 18:43h, 10 JanuaryThank you so much for your response, seriously. I just id the ankle dorsiflexion test. My right knee could touch the wall at 2.5 inches with a “stretch” in the back of my ankle. My left knee could touch the wall at 2.25 inches with a “stretch” in the back of the heel but not as strong a sensation as on the right side. On the left side I also felt something on the bottom of my foot at the metatarsal of my big toe.
I don’t have any muscle weakness. I have developed in the past few days a pain like a small knot in my left hip flexor though I am sure it’s because I’ve been walking like an old person, hunched over so it’s been compressed for sometime, especially since I can’t take normal full length steps. I have had sciatica on my left side on and off for five years whenever I do exercises that work my glute/piriformis.
I haven’t had an MRI yet. I’m traveling the world…I’ve just arrived in one place, Marrakech for a month and I’m due to spend a month in Tunis after this. Not being able to walk is definitely making travel pointless.
I was in Lisbon when it started, which I can understand how this test relates to my condition. It’s very, very hilly there, and I’d been wearing heels which when walking up hill level out the surface, plus my arch was weakened. Then I was wearing flats in that hilly city with uneven cobblestone roads. The flexion on my ankles would have been huge and unprepared for.
I have no other medical conditions. I’m 29.
If I understand your article, I shouldn’t stretch everyday, but three times a week for 5-30 minutes to see if there’s improvement. And does it mean the adhesions are in my ankle? My achilles could have been affected from wearing heels for sure. Or because of how serious it is, do you advise something else? Please help, thank you!
Dareau Debrecen
Posted at 22:35h, 10 JanuaryI actually just noticed that the achilles tendon/area around it on my right side is 25-50% bigger and there is weakness in pointing that foot away from my body in comparison to the left which feels normal. Sigh.
Dr. Chris
Posted at 23:05h, 10 JanuaryI’m going to email you Dareau.
Dareau Debrecen
Posted at 18:27h, 10 JanuaryThank you so much for your response, seriously. I just id the ankle dorsiflexion test. My right knee could touch the wall at 2.5 inches with a “stretch” in the back of my ankle. My left knee could touch the wall at 2.25 inches with a “stretch” in the back of the heel but not as strong a sensation as on the right side. On the left side I also felt something on the bottom of my foot at the metatarsal of my big toe.
I don’t have any muscle weakness. I have developed in the past few days a pain like a small knot in my left hip flexor though I am sure it’s because I’ve been walking like an old person, hunched over so it’s been compressed for sometime, especially since I can’t take normal full length steps. I have had sciatica on my left side on and off for five years whenever I do exercises that work my glute/piriformis.
I haven’t had an MRI yet. I’m traveling the world…I’ve just arrived in one place, Marrakech for a month and I’m due to spend a month in Tunis after this. Not being able to walk is definitely making travel pointless.
I was in Lisbon when it started, which I can understand how this test relates to my condition. It’s very, very hilly there, and I’d been wearing heels which when walking up hill level out the surface, plus my arch was weakened. Then I was wearing flats in that hilly city with uneven cobblestone roads. The flexion on my ankles would have been huge and unprepared for.
I have no other medical conditions. I’m 29.
If I understand your article, I shouldn’t stretch everyday, but three times a week for 5-30 minutes to see if there’s improvement. And does it mean the adhesions are in my ankle? My achilles could have been affected from wearing heels for sure. Or because of how serious it is, do you advise something else? Please help, thank you!